

Commissioner’s Column: Dementia—Options for Paths to Prevention, Detection, and Treatment by Hon. Robert L. Jackson

If you have not read the excellent article in the March/April 2025 Advocate entitled “Balancing the Scales: Practicing Law While Managing Mental Illness,”[1] please do. That anonymous author presented many of the points I had intended to make with this article, but, as it turns out, that previous article serves as a proper introduction for what this article will address.
After reading the March/April article, you know that many types of mental health challenges can affect one’s ability to practice law and do so within the rails of the Idaho Rules of Professional Conduct. This article is intended to address a specific mental health issue—Dementia.
The prevalence of dementia is increasing at an alarming rate. Now, there are over 500,000 new cases a year, just in the United States. That number is expected to reach one million new cases a year by 2050.[2]
This article is not intended to guide an attorney’s decision regarding the timing of retirement. Rather, I hope it will provide some basic information to aid all practitioners, as well as their families, so they can take steps to minimize the effects of dementia later in life and/or deal with their issues now.
Dementia is a general term used to describe a set of symptoms that affect cognitive abilities, memory, thinking, and behavior. It is not a specific disease but rather an umbrella term for a group of symptoms. Alzheimer’s disease is the most common cause of dementia but there are other causes such as vascular dementia, lewy body dementia, frontotemporal dementia (“FTD”), metabolic dementia, traumatic encephalopathy, mechanical, post-radiation, toxins, infections, and dementia caused from tumors.[3]
Why pick dementia as a topic for a bar article? Shouldn’t medical/mental conditions be left to the lawyer, his or her family, and medical providers to deal with? It is, unfortunately, a reality for the population in general and attorneys specifically—out of our Idaho bar population consisting of 6,556, active, house, senior, and judicial members, 3,521 of those, or 53.7 percent are age 50 or older.[4]
Early onset dementia can appear in people of any age. Of course, as one gets older the numbers affected increase. I picked age 50 not because at that age many adults get dementia, but rather, much of the evidence suggests that midlife interventions are important to avoid, reduce, or prolong the onset of symptoms. The earlier one takes care of her or himself, the better the odds for avoiding or prolonging the onset of dementia.
The 2024 report of the Lancet Commission on Dementia Prevention, Intervention, and Care builds upon its 2020 findings by identifying 14 modifiable risk factors associated with dementia across the life course. Notably, in their latest report, the authors introduce two new risk factors: untreated vision loss and high levels of low-density lipoprotein (“LDL”) cholesterol. Their conclusion is, if those factors are addressed, along with the previously identified ones—such as less education, hearing loss, hypertension, smoking, obesity, depression, physical inactivity, diabetes, excessive alcohol consumption, traumatic brain injury, air pollution, and social isolation— there is the potential to prevent or delay approximately 45% of dementia cases.[5]
The Lancet report[6] emphasizes that interventions targeting these 14 risk factors should be tailored to different life stages:
- Early life (0–18 years): Enhancing education to build cognitive reserve.
- Midlife (45–65 years): Managing cardiovascular health, including hypertension and cholesterol levels, and addressing hearing loss.
- Late life (65+ years): Mitigating social isolation and treating vision impairments.
By implementing strategies to modify these risk factors, there is significant potential to reduce the burden of dementia.[7]
John Seelig, MD FAANS, a board certified neurosurgeon and founding member of the Ann Early Intervention Foundation[8] believes that an additional 20 percent of people with dementia symptoms are medically treatable because the source of the symptoms may be vascular, metabolic in nature, may be caused by traumatic encephalopathy, have a genetic basis, a mechanical problem, be neurodegenerative, or may be present because of radiation treatment, toxins, infections, or tumors. There are several excellent newsletters as well as other information which can be found on the Ann Early web site noted above.
If an adult is concerned about the possibility of dementia, several steps can be taken to test for its existence. Here’s a general guide to the process:
1. Consult a Healthcare Professional – But see the caveat below!
- The first step, after considering the above-mentioned caveat, is to visit a doctor. Ideally the doctor will be a neurologist, neuropsychologist or geriatric specialist. They will review the patient’s medical history, current symptoms, and any family history of dementia or related conditions.
2. Cognitive and Memory Tests
- Mini-Mental State Examination (“MMSE”): This is a widely used simple screening tool that can assess various cognitive functions, such as memory, attention, language, and spatial abilities.
- Montreal Cognitive Assessment (“MoCA”): This is another simple screening tool, similar to the MMSE. It may be useful to detect early-stage dementia.
- Other cognitive assessments: There are other cognitive tests which are more than simple screenings. They are validated assessments which are utilized by healthcare professionals to be used as a starting point for diagnosis and treatment. They are Boston Cognitive’s BoCA and Screen, Inc.’s CANS-MCI.
3. Physical and Neurological Exams
- A healthcare professional will conduct a physical and neurological exam to rule out other causes of cognitive decline, such as a stroke, tumor, or other neurological conditions.
- They may assess coordination, muscle strength, reflexes, and other functions that could indicate a neurological issue.
4. Brain Imaging
- Magnetic Resonance Imaging (“MRI”) or Computed Tomography (“CT”) Scans: These can help detect structural changes in the brain that are consistent with dementia, such as atrophy (shrinking) of certain brain regions.
- PET scans: In some cases, Positron Emission Tomography (“PET”) scans can be used to observe patterns of brain activity and detect early signs of Alzheimer’s or other forms of dementia.
5. Blood Tests
- Blood tests can be conducted to rule out other medical conditions that might mimic dementia-like symptoms, such as thyroid problems, vitamin deficiencies, or infections.
- In some cases, blood tests are used to assess biomarkers associated with dementia (e.g., Alzheimer’s disease).
6. Neuropsychological Testing
- A more comprehensive evaluation may involve a neuropsychologist who will conduct in-depth testing to evaluate memory, problem-solving abilities, attention, language, and other cognitive functions. This can help pinpoint the specific cognitive deficits and their severity.
7. Genetic Testing
- In some cases, genetic testing may be done, especially if there’s a strong family history of early-onset dementia. Certain genes, such as the APOE ε4 allele, are associated with an increased risk for Alzheimer’s disease, though not all individuals with this gene will develop the condition.
8. Evaluate Daily Functioning
- Often, dementia is diagnosed when changes in a person’s ability to perform everyday tasks (e.g., managing finances, driving, or handling daily chores) become apparent. Tracking the progression of difficulties in these areas can help doctors assess the severity and nature of cognitive decline.
9. Monitor Symptoms Over Time
- Since dementia progresses slowly, sometimes symptoms may need to be monitored over a longer period of time. Regular check-ups will help assess the rate of cognitive decline and the appropriate course of action.
If someone suspects dementia, early detection can significantly help with managing the condition and exploring potential treatment options. If you or someone you know is experiencing symptoms of cognitive decline, seeking medical advice as soon as possible is essential.
CAVEAT. There is a major consideration to contemplate before you see a doctor!
As discussed in the anonymous March/April Advocate article, what happens if your friends, your clients, your doctor, your insurance company, the bar, the DMV, any licensing agencies etc. believe you have dementia? The risk of stigma and misunderstanding could unnecessarily jeopardize your reputation, career trajectory, income, the cost of insurance or the ability to even get insurance.
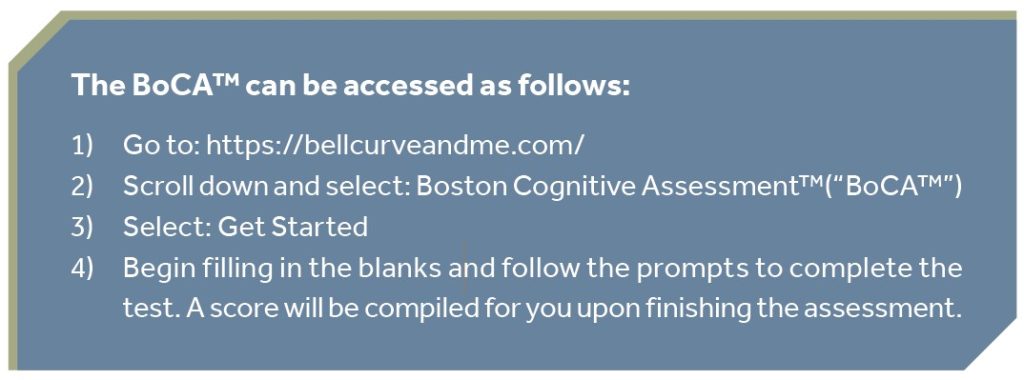
One approach to take, if one is not sure how his or her mental capacity stacks up against others, is to do some anonymous testing. There are several options available with a simple google search. One I am familiar with is produced by Boston Cognitive. The Boston Cognitive test can be taken anywhere and is called the Boston Cognitive Assessment (“BoCA”). It can be completed in about 10 minutes and provides a raw score of 0-30, with a secondary score that compares your score to your peers. Once one has a test result, she or he can consider the next step which could be anything from doing nothing to an appointment with a neurosurgeon.
Whatever your score, the beauty of the self-administered BoCA is the privacy of the result. Certainly, it is not to be used as a determination of one’s fitness to practice law. However, it can provide guidance for your next steps in life. Those steps may be: consulting with your physician, calling the Department of Veteran Affairs if you qualify, contacting your local Alzheimer’s Association Chapter, or, if you want to consult with a physician who participated in the clinical trials for the BoCA, contact Dr. Mikhail Kogan. He is the Chief Medical Officer at the George Washington Center for Integrative Medicine.[9] Another option could be to contact the previously noted Dr. John Seelig.[10]
In closing, an important point I want to make is that you should not give up. For the younger individuals, take control and heed those 14 factors as described in the Lancet Commission 2024 report discussed previously. For those who are older—it is never too late to adjust one’s behavior or habits.
Science is making new and exciting discoveries all the time. For example, sensory therapy utilizing 40 Hz light and sound has shown promise in improving cognition. There is an excellent app available from your app stores called “AlzLife” if you are inclined to explore that.[11] There are new medications being developed. The Alzheimer’s Association web site contains a wealth of knowledge and options—for any type of dementia-related issues.
Dementia is something that, if we live long enough, we will probably all experience. Early detection is key. Regular testing is key. Get that baseline score and monitor it for your health and your decision regarding when it may become time to give up the practice!
__________________________________________________________________________
The author wishes to thank John M. Seelig, MD, FAANS, Neurosurgeon, La Jolla, California and Kevin Wolfe, Director of Customer Solutions with Boston Cognitive, (414-807-5397; kevin.wolfe@bostoncognitive.com) for their help and contributions in preparing this article.
Judge Robert L. Jackson practiced law in Idaho from 1983 until going on the bench as a magistrate in Payette County in August 2013. His varied practice included criminal prosecution, criminal defense, assistant city attorney, personal injury (plaintiff and defense), medical malpractice, insurance law, and workers’ compensation. Judge Jackson also serves as the Idaho State Bar Commissioner representing the Third and Fifth Districts. When not engaged in legal work you can find him, with family members or friends, at a concert, hiking, backpacking, farming, or traveling.
[1] Anonymous, Balancing the Scales: Practicing Law While Managing Mental Illness, 68 The Advocate 24 (2025).
[2] Jocelyn Solis-Moreira, Two in Five Americans Are at Lifetime Risk of Dementia after Age 55, Researchers Warn, Scientific American, https://www.scientificamerican.com/article/annual-u-s-dementia-cases-projected-to-rise-to-1-million-by-2060/ (last visited Apr 4, 2025).
[3] Alzheimer’s Vs Dementia – What’s The Difference?, UCLA Medical School (2023), https://medschool.ucla.edu/news-article/alzheimers-vs-dementia-what-is-the-difference (last visited Apr 17, 2025).
[4] Idaho State Bar Membership Data (Accessed March 14, 2025).
[5] Gill Livingston et al., Dementia Prevention, Intervention, and Care: 2024 Report of the Lancet Standing Commission, 404 The Lancet 572 (2024).
[6] Id.
[7] For a graphic representing this, see this endnote. ADI – Lancet Commission identifies two new risk factors for dementia and suggests 45% of cases could be delayed or reduced, https://www.alzint.org/news-events/news/lancet-commission-identifies-two-new-risk-factors-for-dementia-and-suggests-45-of-cases-could-be-delayed-or-reduced/ (last visited Apr 17, 2025).
[8] Ann Early Intervention Foundation, Ann Early Intervention Foundation, https://www.annearlyintervention.org (last visited Apr 22, 2025).
[9] GW Center for Integrative Medicine, GW Center For Integrative Medicine (2025), https://gwcim.com/ (last visited Apr 22, 2025).
[10] He can be reached via email at jseelig12@gmail.com or texted at 858-395-2300. If you text be sure you explain the purpose of your inquiry.
[11] Sienna D. McNett et al., A Feasibility Study of AlzLife 40 Hz Sensory Therapy in Patients with MCI and Early AD, 11 Healthcare 2040 (2023).